Diabetes doesn’t just affect your blood sugar-it slowly damages the tiny blood vessels in your eyes. This condition is called diabetic retinopathy, and it’s the leading cause of vision loss in adults between 21 and 64 in the U.S. The scary part? You might not notice any symptoms until the damage is serious-and irreversible.
How Diabetic Retinopathy Starts
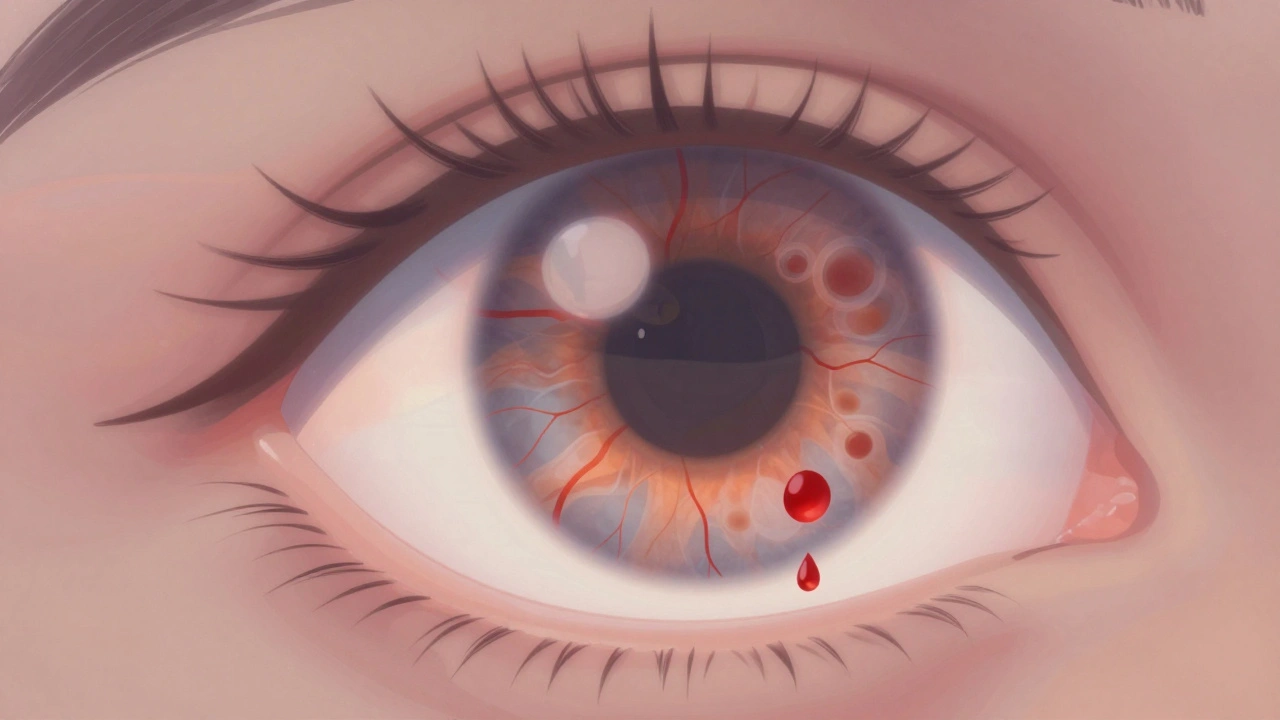
When blood sugar stays high for years, it wears down the walls of the blood vessels in your retina. The retina is the light-sensitive layer at the back of your eye that turns images into signals your brain understands. Over time, these weakened vessels start to leak fluid or bleed. Sometimes, they even close off completely, starving parts of the retina of oxygen. In response, your eye tries to fix the problem by growing new blood vessels. But these aren’t normal. They’re fragile, messy, and prone to bursting. When they bleed, you might see dark spots or floaters floating across your vision. If they pull on the retina, it can detach-like wallpaper peeling off a wall. That’s when vision loss becomes sudden and severe. There are three clear stages:- Mild nonproliferative: Small bulges called microaneurysms form in vessel walls. No symptoms yet.
- Moderate to severe nonproliferative: More vessels are blocked. Fluid leaks into the retina, causing swelling-especially in the macula, the part responsible for sharp central vision. This is called diabetic macular edema (DME), and it affects about 1 in 15 people with diabetes.
- Proliferative: New, abnormal blood vessels grow on the retina’s surface. These can bleed into the vitreous (the gel inside your eye), cause scarring, or pull the retina loose.
Why You Might Not Know You Have It
This is the biggest danger: diabetic retinopathy doesn’t hurt. It doesn’t make your eyes red. It doesn’t cause pain or itching. For most people, vision stays perfectly normal-even as damage builds up. Studies show that nearly 70% of patients only notice symptoms when the condition is already moderate or worse. Common signs include:- Blurred or wavy vision
- Floaters or dark spots that won’t go away
- Difficulty seeing at night or in low light
- Fading or washed-out colors
- Loss of side vision
Laser Treatment: How It Works
Laser treatment-also called photocoagulation-is one of the oldest and most proven ways to stop diabetic retinopathy from stealing your vision. It’s not a cure, but it’s highly effective at slowing or stopping progression. There are two main types:- Focal laser: Used for diabetic macular edema. The laser targets specific leaking blood vessels near the macula to seal them and reduce swelling.
- Scatter laser (panretinal photocoagulation): Used for proliferative retinopathy. Instead of targeting one spot, the laser makes hundreds of tiny burns across the peripheral retina. This stops the retina from sending signals to grow new, abnormal blood vessels.

What Laser Treatment Can’t Fix
If fluid has already caused permanent scarring in the macula, or if the retina has detached, laser alone won’t bring back your sight. In those cases, you might need a vitrectomy-surgery to remove blood or scar tissue from inside the eye. Laser treatment also has side effects:- Reduced night vision
- Loss of peripheral vision (especially after scatter laser)
- Blurred vision for a few days after the procedure
The Real Key: Managing Diabetes
Laser treatment works best when paired with tight blood sugar control. Research from the Cleveland Clinic shows that keeping your HbA1c levels below 7% can cut the risk of retinopathy progression by up to 76%. That’s not a small number-it’s life-changing. High blood pressure and high cholesterol make retinopathy worse. Smoking doubles your risk. Pregnancy can trigger rapid progression in women with diabetes. The truth is, no laser in the world can outwork poor diabetes management. If your blood sugar is all over the place, even the best eye treatment will struggle to keep up.
Screening: The Only Reliable Defense
The American Diabetes Association and the NHS both recommend a comprehensive dilated eye exam at least once a year for everyone with diabetes. If you already have retinopathy, you may need exams every few months. These aren’t optional checkups-they’re survival tools. A simple retinal photo can catch early damage before you feel anything. Newer tools, like AI-powered imaging, are making screening faster and more accurate. Some clinics even offer remote screenings using digital cameras you can use at your primary care doctor’s office. Don’t wait for blurry vision. Don’t wait for floaters. Don’t wait for a doctor to say something’s wrong. If you have diabetes, your eyes need to be checked-every single year.What’s Next? New Treatments on the Horizon
Laser treatment isn’t going away, but it’s no longer the only option. Anti-VEGF injections-medications like ranibizumab and aflibercept-are now used to treat diabetic macular edema and sometimes proliferative retinopathy. These injections block a protein called VEGF that tells the eye to grow abnormal blood vessels. They’re given as tiny shots into the eye, usually every 4 to 8 weeks. Many patients see improved vision after just a few treatments. The trend now is combination therapy: laser to stabilize the retina, plus injections to reduce swelling. This approach gives better results than either treatment alone. Research is also exploring longer-lasting drugs and even gene therapies that could one day stop the damage at its source. But for now, the best defense is still simple: know your numbers, get your eyes checked, and don’t ignore the silent warning signs.Can diabetic retinopathy be reversed?
No, once retinal tissue is damaged or scarred, the vision loss can’t be undone. But early treatment can stop the damage from getting worse. That’s why regular eye exams are so important-they catch problems before they become permanent.
How often should I get my eyes checked if I have diabetes?
Once a year is the standard recommendation. If you already have signs of retinopathy, your eye doctor may ask you to come back every 3 to 6 months. Pregnant women with diabetes should have an exam in the first trimester and possibly again later in pregnancy, since hormonal changes can speed up retinopathy.
Does laser treatment hurt?
Most people feel a mild pressure or a quick pinch during the procedure. Numbing drops are used, so you won’t feel pain. Afterward, your vision might be blurry for a few hours, and you’ll need someone to drive you home. Some people report mild discomfort or sensitivity to light for a day or two.
Can I prevent diabetic retinopathy entirely?
You can’t guarantee you’ll never get it, but you can dramatically lower your risk. Keep your blood sugar, blood pressure, and cholesterol under control. Don’t smoke. Get yearly eye exams. Studies show that people who manage their diabetes well reduce their risk of vision loss by more than 75%.
Are there alternatives to laser treatment?
Yes. Anti-VEGF injections are now the first-line treatment for diabetic macular edema. They’re often used before or instead of laser, especially when swelling is the main problem. For advanced cases, surgery (vitrectomy) may be needed to remove blood or scar tissue. Laser is still used, but now it’s often part of a combination plan.




nikki yamashita
December 13, 2025 AT 05:51Just got my annual eye exam last week-thank god I went. No signs yet, but my doc said I’m lucky. If you have diabetes, don’t be like me and wait until you’re scared. Go now. Seriously.
Adam Everitt
December 13, 2025 AT 20:00laser? i thought they just poked ur eyes with a light saber or sumthin. jk… kinda. but like… why does it hurt so much if its just light? 🤔
Reshma Sinha
December 15, 2025 AT 16:50Diabetic retinopathy progression is directly correlated with glycemic variability and chronic hyperglycemia-HbA1c >7% significantly upregulates VEGF expression, triggering neovascularization. Early intervention with panretinal photocoagulation remains gold standard for proliferative DR, but adjunctive anti-VEGF therapy is now preferred for DME due to superior visual acuity outcomes.
Lawrence Armstrong
December 16, 2025 AT 12:27Been there. Got the laser. Lost some peripheral vision but kept my central sight. 😌 Worth it. Don’t wait. Get checked. Period. 🙏
Audrey Crothers
December 16, 2025 AT 21:56MY EYES ARE MY MOST VALUABLE ASSET AND I’M NOT LETTING DIABETES STEAL THEM 😭 I get checked every 6 months now and my A1c is 6.2! If I can do it, YOU CAN TOO!!
Stacy Foster
December 18, 2025 AT 18:07They’re not telling you the whole truth about lasers. Did you know the FDA approved these procedures without long-term studies? They’re just trying to keep you dependent on eye clinics while Big Pharma profits from injections. You’re being manipulated.
Donna Anderson
December 19, 2025 AT 23:54i didnt even know this was a thing until my cousin lost sight in one eye. now i check my sugar like its my job. and i make my dad go to the eye doc every year. he hates it but he goes. lol
sandeep sanigarapu
December 20, 2025 AT 17:38Diabetes is a systemic disease. The eye is merely the messenger. Prevention lies in disciplined lifestyle, not reactive interventions. Annual screening is non-negotiable. Discipline over desperation.
Ashley Skipp
December 21, 2025 AT 07:28Why do people ignore this until it’s too late? It’s not rocket science. Control sugar. Get checked. Don’t be dumb. End of story.
Nathan Fatal
December 22, 2025 AT 16:07There’s a deeper truth here: vision loss from diabetes isn’t just medical-it’s existential. It forces us to confront the fragility of control. We manage glucose to avoid chaos, but the body remembers every spike. The laser doesn’t heal-it’s a ceasefire. The real war is in the daily choices.
wendy b
December 22, 2025 AT 23:26Actually the studies cited are outdated. The 2023 Cochrane Review showed anti-VEGF is superior in 89% of cases. Also, laser causes more neurodegeneration than previously thought. You’re being sold a 1980s solution.
Robert Webb
December 23, 2025 AT 17:29I’ve been a diabetes educator for 18 years and I can’t stress this enough: people think they’re fine because they ‘feel okay.’ But your body doesn’t feel glucose levels-it just accumulates damage. That’s why the silent progression is so dangerous. It’s not dramatic. It’s quiet. And that’s why we lose people. Not because they’re lazy, but because they don’t know what they don’t know. The eye exam isn’t optional-it’s your body’s last whisper before it screams.
Rob Purvis
December 24, 2025 AT 09:33Just want to add: if you’re on insulin, your risk is higher-but so is your control potential. Tight management = lower risk. Also, wear sunglasses. UV exposure worsens retinal stress. And hydrate. Seriously. Dehydration thickens blood. More strain on capillaries. Small things matter.
Laura Weemering
December 25, 2025 AT 19:53They’re all lying. The real cause is glyphosate in our food supply. The FDA knows. The AMA knows. But they won’t tell you because the pharmaceutical-industrial complex depends on chronic disease. Your retina is a canary in the coal mine. And they’re poisoning the mine.